What Are Bursitis Of The Foot Conditions
Overview
Retrocalcaneal bursitis is the inflammation of the retrocalcaneal bursa, which is located behind the heel bone, also known as the calcaneal bone (hence the name retrocalcaneal). The retrocalcaneal bursa is a thin, slippery, fluid-filled sac that serves as a both a cushion and lubricant between the heel bone and the Achilles tendon. Inflammation of the retrocalcaneal bursa usually results from irritation of the bursa. This irritation may be due to certain activities, an underlying health condition such as arthritis, or an abnormality of the foot, such the development of a boney prominence on the calcaneal bone, called a Haglund's deformity.
Causes
The most common causative organism is Staphylococcus aureus (80% of cases), followed by streptococci. However, many other organisms have been implicated in septic bursitis, including mycobacteria (both tuberculous and nontuberculous strains), fungi (Candida), and algae (Prototheca wickerhamii). Factors predisposing to infection include diabetes mellitus, steroid therapy, uremia, alcoholism, skin disease, and trauma. A history of noninfectious inflammation of the bursa also increases the risk of septic bursitis.
Symptoms
Where the tendon joins the calcaneal bone, friction can cause the spaces between the tendon, bone and skin to swell and inflame with bursitis. This constitutes a calcaneal bursa. Apart from swelling over the back of the heel, you?ll feel acute tenderness and pain when you move it or even apply light pressure. Your swollen heel may look more red than the other one, and the swelling is often so hard it can feel like bone, partly because it sometimes is, as a bony overgrowth can occur in chronic cases.
Diagnosis
Before making a diagnosis of retrocalcaneal bursitis, a doctor must rule out other possible problems, such as arthritis, a fracture or tumor. A doctor also will try to determine if the Achilles tendon itself is a source of pain. To make a diagnosis, a doctor will use some or all of the diagnostic tools below Patient interview. A doctor will ask a patient about medical history, and to describe the onset of his or her symptoms, the pattern of pain and swelling, and how symptoms affect lifestyle. For example, doctors may ask patients what types of shoes they wear and what they do for exercise. A patient's reported symptoms are important to diagnosis and treatment. The doctor will also ask what home treatments have helped the condition. Physical exam. A doctor will examine the patient's foot, noting swelling, tenderness and pain points, and range of motion. The doctor also may ask the patient to point and flex the feet and stand on his or her toes.
Non Surgical Treatment
Despite appropriate physiotherapy management, some patients with retrocalcaneal bursitis do not improve adequately. When this occurs the treating physiotherapist or doctor can advise on the best course of management. This may include further investigations such as an ultrasound, X-Ray, MRI or CT scan, pharmaceutical intervention, corticosteroid and anaesthetic injection into the retrocalcaneal bursa, draining of the bursa, or review by a specialist or podiatrist who can advise on any treatment that may be appropriate to improve the condition.
Surgical Treatment
Bursectomy is a surgical procedure used to remove an inflamed or infected bursa, which is a fluid-filled sac that reduces friction between tissues of the body. Because retrocalcaneal bursitis can cause chronic inflammation, pain and discomfort, bursectomy may be used as a treatment for the condition when it is persistent and cannot be relived with other treatments. During this procedure, a surgeon makes small incisions so that a camera may be inserted into the joint. This camera is called an arthroscope. Another small incision is made so that surgical instruments can be inserted to remove the inflamed bursa.
Retrocalcaneal bursitis is the inflammation of the retrocalcaneal bursa, which is located behind the heel bone, also known as the calcaneal bone (hence the name retrocalcaneal). The retrocalcaneal bursa is a thin, slippery, fluid-filled sac that serves as a both a cushion and lubricant between the heel bone and the Achilles tendon. Inflammation of the retrocalcaneal bursa usually results from irritation of the bursa. This irritation may be due to certain activities, an underlying health condition such as arthritis, or an abnormality of the foot, such the development of a boney prominence on the calcaneal bone, called a Haglund's deformity.
Causes
The most common causative organism is Staphylococcus aureus (80% of cases), followed by streptococci. However, many other organisms have been implicated in septic bursitis, including mycobacteria (both tuberculous and nontuberculous strains), fungi (Candida), and algae (Prototheca wickerhamii). Factors predisposing to infection include diabetes mellitus, steroid therapy, uremia, alcoholism, skin disease, and trauma. A history of noninfectious inflammation of the bursa also increases the risk of septic bursitis.
Symptoms
Where the tendon joins the calcaneal bone, friction can cause the spaces between the tendon, bone and skin to swell and inflame with bursitis. This constitutes a calcaneal bursa. Apart from swelling over the back of the heel, you?ll feel acute tenderness and pain when you move it or even apply light pressure. Your swollen heel may look more red than the other one, and the swelling is often so hard it can feel like bone, partly because it sometimes is, as a bony overgrowth can occur in chronic cases.
Diagnosis
Before making a diagnosis of retrocalcaneal bursitis, a doctor must rule out other possible problems, such as arthritis, a fracture or tumor. A doctor also will try to determine if the Achilles tendon itself is a source of pain. To make a diagnosis, a doctor will use some or all of the diagnostic tools below Patient interview. A doctor will ask a patient about medical history, and to describe the onset of his or her symptoms, the pattern of pain and swelling, and how symptoms affect lifestyle. For example, doctors may ask patients what types of shoes they wear and what they do for exercise. A patient's reported symptoms are important to diagnosis and treatment. The doctor will also ask what home treatments have helped the condition. Physical exam. A doctor will examine the patient's foot, noting swelling, tenderness and pain points, and range of motion. The doctor also may ask the patient to point and flex the feet and stand on his or her toes.
Non Surgical Treatment
Despite appropriate physiotherapy management, some patients with retrocalcaneal bursitis do not improve adequately. When this occurs the treating physiotherapist or doctor can advise on the best course of management. This may include further investigations such as an ultrasound, X-Ray, MRI or CT scan, pharmaceutical intervention, corticosteroid and anaesthetic injection into the retrocalcaneal bursa, draining of the bursa, or review by a specialist or podiatrist who can advise on any treatment that may be appropriate to improve the condition.
Surgical Treatment
Bursectomy is a surgical procedure used to remove an inflamed or infected bursa, which is a fluid-filled sac that reduces friction between tissues of the body. Because retrocalcaneal bursitis can cause chronic inflammation, pain and discomfort, bursectomy may be used as a treatment for the condition when it is persistent and cannot be relived with other treatments. During this procedure, a surgeon makes small incisions so that a camera may be inserted into the joint. This camera is called an arthroscope. Another small incision is made so that surgical instruments can be inserted to remove the inflamed bursa.
Hammer Toe Pain
 Overview
Overview
Hammer toes are usually not a serious condition, but can become painful as the bent joint rubs against the inside of the shoe, causing irritation, corns, or calluses on the top of the middle joint or the tip of the toe. A Hammer toe may also cause occasional shooting pains throughout the toes or elsewhere in the foot. A hammertoe has a kink or contracture in its second joint--called the proximal interphalangeal joint--that causes the toe to bend upward in the middle, giving it a hammer-like appearance. The raised part of the toe often rubs on shoes, leading to the formation of corns or calluses. Usually hammertoe affects the smaller toes, causing pain and interfering with the ability to walk normally.
Causes
Those fashionable shoes. Women tend to cram their feet into too-narrow, ill-fitting shoes with little to no arch support. That?s why we see more hammertoes in women than men. Pointy, high-heeled shoes put severe pressure on the toes and their joints, and they typically have little to no arch support. Neuromuscular diseases can contribute to the development of hammertoe, too. People with diabetes can be at increased risk for complications from a hammertoe. In diabetics, if a toe has a corn or other ulceration, it indicates there is too much pressure on the toes. In those with poor blood flow or neuropathy, these lesions can get infected and lead to the loss of a toe or foot unless shoes are modified.
 Symptoms
Symptoms
Common symptoms of hammertoes include pain or irritation of the affected toe when wearing shoes. corns and calluses (a buildup of skin) on the Hammer toes toe, between two toes, or on the ball of the foot. Corns are caused by constant friction against the shoe. They may be soft or hard, depending upon their location. Inflammation, redness, or a burning sensation. Contracture of the toe. In more severe cases of hammertoe, open sores may form.
Diagnosis
Your healthcare provider will examine your foot, checking for redness, swelling, corns, and calluses. Your provider will also measure the flexibility of your toes and test how much feeling you have in your toes. You may have blood tests to check for arthritis, diabetes, and infection.
Non Surgical Treatment
Mild hammer toe in children can be treated by manipulating and splinting the affected toe. The following changes in footwear may help relieve symptoms. Wear the right size shoes or shoes with wide toe boxes for comfort, and to avoid making hammer toe worse. Avoid high heels as much as possible. Wear soft insoles to relieve pressure on the toe. Protect the joint that is sticking out with corn pads or felt pads. A foot doctor can make foot devices called hammer toe regulators or straighteners for you, or you can buy them at the store. Exercises may be helpful. You can try gentle stretching exercises if the toe is not already in a fixed position. PIcking up a towel with your toes can help stretch and straighten the small muscles in the foot.
Surgical Treatment
Extreme occurrences of hammer toe may call for surgery. Your surgeon will decide which form of surgery will best suit your case. Often, the surgeon may have to cut or remove a tendon or ligament. Depending on the severity of your condition, the bones on both sides of the joint afflicted may need to be fused together. The good news is you can probably have your surgery and be released to go home in one day. You will probably experience some stiffness in your toe, but it might last for a short period, then your long-term pain will be eliminated.
Over-Pronation Of The Foot What Are The Symptoms
Overview
Pronation is the normal movement the foot makes to absorb the impact from walking or running. It occurs once the heel strikes the ground and the foot disperses the impact, stretching and flattening the arch as the foot rolls inward. Supination is the opposite motion of pronation. The foot supinates, or rolls on its outer edge, to help with stability as we walk or run. A reasonable amount of pronation is necessary for the foot to function properly. However, when the foot arch remains flat and the foot rolls inward too much one may have excessive pronation or overpronation. This medical condition can result from continually straining the feet and wearing footwear that lacks sufficient foot arch support.
Causes
Pronation can occur as an overuse syndrome in active runners, where a great deal of stress is placed on ligaments and tendons that support the medial column. Obesity is another predictor for pronation and deterioration of the medial ligaments and posterior tibial tendon due to excessive stress on these tissues. Acute Trauma can also lead to over-pronation when ligaments are torn or tendon is ruptured. Once again this can lead to a collapse of the medial column. Arthritic conditions involving the knee joint when the joint is in varus (inner collapse) posture, this places the center of gravity over the ankle joint rather than the foot causing undue pressure on the inner ankle.
Symptoms
In addition to problems overpronation causes in the feet, it can also create issues in the calf muscles and lower legs. The calf muscles, which attach to the heel via the Achilles tendon, can become twisted and irritated as a result of the heel rolling excessively toward the midline of the body. Over time this can lead to inflexibility of the calf muscles and the Achilles tendon, which will likely lead to another common problem in the foot and ankle complex, the inability to dorsiflex. As such, overpronation is intrinsically linked to the inability to dorsiflex.
Diagnosis
The best way to discover whether you have a normal gait, or if you overpronate, is to visit a specialty run shop, an exercise physiologist, a podiatrist or a physical therapist who specializes in working with athletes. A professional can analyze your gait, by watching you either walk or run, preferably on a treadmill. Some facilities can videotape your gait, then analyze the movement of your feet in slow-motion. Another (and less costly) way is to look at the bottom of an older pair of run shoes. Check the wear pattern. A person with a normal gait will generally see wear evenly across the heel and front of the shoe. A person who overpronates will likely see more wear on the OUTside of the heel and more wear on the INside of the forefoot (at the ball). A person who supinates will see wear all along the outer edges of the shoe. You can also learn about your gait by looking at your arches. Look at the shape your wet feet leave on a piece of paper or a flat walking surface.
Non Surgical Treatment
An overpronator is a person who overpronates, meaning that when walking or running their feet tend to roll inwards to an excessive degree. Overpronation involves excessive flattening of the arches of the feet, with the roll seeing the push off take place from the inside edge of the foot and the big toe. When this happens, the muscles and ligaments in the feet are placed under excessive strain, which can lead to pain and premature fatigue of the foot. Overpronation is most commonly experienced in people who have flat feet or fallen arches.
Surgical Treatment
Calcaneal "Slide" (Sliding Calcaneal Osteotomy) A wedge is cut into the heel bone (calcaneus) and a fixation device (screws, plate) is used to hold the bone in its new position. This is an aggressive option with a prolonged period of non-weightbearing, long recovery times and many potential complications. However, it can and has provided for successful patient outcomes.
Pronation is the normal movement the foot makes to absorb the impact from walking or running. It occurs once the heel strikes the ground and the foot disperses the impact, stretching and flattening the arch as the foot rolls inward. Supination is the opposite motion of pronation. The foot supinates, or rolls on its outer edge, to help with stability as we walk or run. A reasonable amount of pronation is necessary for the foot to function properly. However, when the foot arch remains flat and the foot rolls inward too much one may have excessive pronation or overpronation. This medical condition can result from continually straining the feet and wearing footwear that lacks sufficient foot arch support.
Causes
Pronation can occur as an overuse syndrome in active runners, where a great deal of stress is placed on ligaments and tendons that support the medial column. Obesity is another predictor for pronation and deterioration of the medial ligaments and posterior tibial tendon due to excessive stress on these tissues. Acute Trauma can also lead to over-pronation when ligaments are torn or tendon is ruptured. Once again this can lead to a collapse of the medial column. Arthritic conditions involving the knee joint when the joint is in varus (inner collapse) posture, this places the center of gravity over the ankle joint rather than the foot causing undue pressure on the inner ankle.
Symptoms
In addition to problems overpronation causes in the feet, it can also create issues in the calf muscles and lower legs. The calf muscles, which attach to the heel via the Achilles tendon, can become twisted and irritated as a result of the heel rolling excessively toward the midline of the body. Over time this can lead to inflexibility of the calf muscles and the Achilles tendon, which will likely lead to another common problem in the foot and ankle complex, the inability to dorsiflex. As such, overpronation is intrinsically linked to the inability to dorsiflex.
Diagnosis
The best way to discover whether you have a normal gait, or if you overpronate, is to visit a specialty run shop, an exercise physiologist, a podiatrist or a physical therapist who specializes in working with athletes. A professional can analyze your gait, by watching you either walk or run, preferably on a treadmill. Some facilities can videotape your gait, then analyze the movement of your feet in slow-motion. Another (and less costly) way is to look at the bottom of an older pair of run shoes. Check the wear pattern. A person with a normal gait will generally see wear evenly across the heel and front of the shoe. A person who overpronates will likely see more wear on the OUTside of the heel and more wear on the INside of the forefoot (at the ball). A person who supinates will see wear all along the outer edges of the shoe. You can also learn about your gait by looking at your arches. Look at the shape your wet feet leave on a piece of paper or a flat walking surface.
Non Surgical Treatment
An overpronator is a person who overpronates, meaning that when walking or running their feet tend to roll inwards to an excessive degree. Overpronation involves excessive flattening of the arches of the feet, with the roll seeing the push off take place from the inside edge of the foot and the big toe. When this happens, the muscles and ligaments in the feet are placed under excessive strain, which can lead to pain and premature fatigue of the foot. Overpronation is most commonly experienced in people who have flat feet or fallen arches.
Surgical Treatment
Calcaneal "Slide" (Sliding Calcaneal Osteotomy) A wedge is cut into the heel bone (calcaneus) and a fixation device (screws, plate) is used to hold the bone in its new position. This is an aggressive option with a prolonged period of non-weightbearing, long recovery times and many potential complications. However, it can and has provided for successful patient outcomes.
Treating Calcaneal Apophysitis
Overview
Sever's Disease is a serious type of 'growing pain' rooted in the fact that the rate of growth of a child's heel bones is slower than that of the ligaments of the leg. The heel bone is one of the first bones in the human body to reach full size, and it is prone to injury because it is not flexible or elastic. As a child goes through growth spurts of the heel bone, the Achilles tendon, which connects the calf muscle to the heel, may be struggling to play catch-up, due to its slower rate of growth. In this scenario, the tendon and leg muscles can become strained, tight and over-stretched. As the child walks, runs or plays, repetitive pressure is placed on the tendon, and the tension can cause damage to the growing heel bone, resulting in pain and inflammation.
Causes
There is no specific known cause of Sever?s disease. However, there are several common factors associated with the condition including. Tight calf muscles. Pronated foot type (rolled in towards the ankle). Children who are heavier. Puberty/growth spurts. External factors, e.g. hard surfaces or poor footwear. Increase in physical activity levels.
Symptoms
The pain associated with Sever's disease is usually felt along the back of the heel and becomes worse when running or walking. In some children, the pain is so severe they may limp when walking. One of the diagnostic tests for Sever's disease is the "squeeze test". Squeezing both sides of the heel together will produce immediate discomfort. Many children feel pain immediately upon waking and may have calf muscle stiffness in the morning.
Diagnosis
You may have pain when your doctor squeezes your heel bone. You may have pain when asked to stand or walk on your toes or on your heels. You may have pain in your heel when your doctor stretches your calf muscles. Your doctor may order x-rays of the injured foot to show an active growth plate.
Non Surgical Treatment
Physiotherapy treatment to improve range of the ankle and descrease soft tissue tightness. Orthotics to control excessive motion of the foot. Icing the painful area. Use of topical anti-inflammatory cream. Taping of the foot during exercise. Stretching, only if recommended by the physiotherapist.
Recovery
Severs disease is a self limiting condition that gradually resolves as the patient moves towards skeletal maturity. This usually takes between 6 to 12 months, but may persist for as long as 2 years. With appropriate management, symptoms may resolve in a number of weeks. Patients with Severs disease typically improve gradually over time and full function is restored.
Sever's Disease is a serious type of 'growing pain' rooted in the fact that the rate of growth of a child's heel bones is slower than that of the ligaments of the leg. The heel bone is one of the first bones in the human body to reach full size, and it is prone to injury because it is not flexible or elastic. As a child goes through growth spurts of the heel bone, the Achilles tendon, which connects the calf muscle to the heel, may be struggling to play catch-up, due to its slower rate of growth. In this scenario, the tendon and leg muscles can become strained, tight and over-stretched. As the child walks, runs or plays, repetitive pressure is placed on the tendon, and the tension can cause damage to the growing heel bone, resulting in pain and inflammation.
Causes
There is no specific known cause of Sever?s disease. However, there are several common factors associated with the condition including. Tight calf muscles. Pronated foot type (rolled in towards the ankle). Children who are heavier. Puberty/growth spurts. External factors, e.g. hard surfaces or poor footwear. Increase in physical activity levels.
Symptoms
The pain associated with Sever's disease is usually felt along the back of the heel and becomes worse when running or walking. In some children, the pain is so severe they may limp when walking. One of the diagnostic tests for Sever's disease is the "squeeze test". Squeezing both sides of the heel together will produce immediate discomfort. Many children feel pain immediately upon waking and may have calf muscle stiffness in the morning.
Diagnosis
You may have pain when your doctor squeezes your heel bone. You may have pain when asked to stand or walk on your toes or on your heels. You may have pain in your heel when your doctor stretches your calf muscles. Your doctor may order x-rays of the injured foot to show an active growth plate.
Non Surgical Treatment
Physiotherapy treatment to improve range of the ankle and descrease soft tissue tightness. Orthotics to control excessive motion of the foot. Icing the painful area. Use of topical anti-inflammatory cream. Taping of the foot during exercise. Stretching, only if recommended by the physiotherapist.
Recovery
Severs disease is a self limiting condition that gradually resolves as the patient moves towards skeletal maturity. This usually takes between 6 to 12 months, but may persist for as long as 2 years. With appropriate management, symptoms may resolve in a number of weeks. Patients with Severs disease typically improve gradually over time and full function is restored.
Fallen Arch Pain Relief
Overview
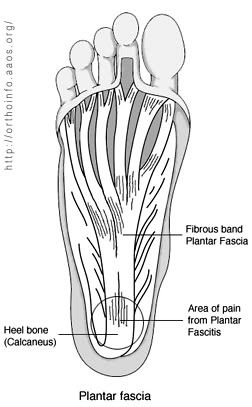
Arch pain is felt on the underside of your foot between the heel and ball. The purpose of the arch is to transfer your body weight from heel to toe, and pain is the result when the arch doesn?t function properly. Your foot actually contains two arches: the longitudinal arch which runs the length of your foot, and the transverse arch (also known as the metatarsal arch) which spans the width of your foot. There are 24 bones which create the arches and these bones are held together through their unique interlocking shapes and ligaments. The muscles and the plantar fascia (a broad band of fibrous tissue which runs from the heel to the toes) provide secondary support, and fat pads help to absorb impact and bear your weight. If any of these structures or their interaction are damaged or faulty, arch pain may occur. The most common cause of arch pain is plantar fasciitis, an inflammation of the plantar fascia. You may also suffer arch pain if you have a structural imbalance in your foot or suffer from arthritis. But arch pain may also result from stepping on a rock or when someone steps on your foot. This force may cause an injury such as a bone fracture or damage to the supporting muscles, ligaments, or tendons underneath your foot.
Causes
Spending a lot of time on your feet. Especially when you are not used to doing so. For example you may have started a new job such as waiting tables where you are on your feet all day and wake up the next day with sore feet. This is a sign of damage and over time could lead to plantar fasciitis. Being Over-Weight. Never an easy topic to discuss but in simple terms, the heavier you are, the greater the burden on your feet. There are times when you're walking when your entire body weight is borne on one leg and therefore one foot, placing great strain on the plantar fascia. Wearing shoes with poor arch support or cushioning. A tight Achilles tendon. This is the big tendon at the bottom of your calf muscles above your heel. If this is excessively tight this can affect your ability to flex your ankle and make you more likely to damage your plantar fascia. Suddenly changing your exercise routine. Using running as an example if you suddenly run many more miles than your are used to or change to a new running surface e.g. grass to tarmac - these factors can put excessive strain on the plantar fascia and lead to plantar fasciitis. All of these risk factors ultimately lead to a specific change in foot structure. The term given is over-pronation and this basically describes rolling in of the foot and lowering of the arches. It is this change that excessively elongates the plantar fascia which can lead to plantar fasciitis.
Symptoms
Common symptoms of plantar fasciitis include pain in the morning when you first get out of bed, pain and stiffness when you start to walk after sitting for a while, increasing arch or heel pain toward the end of the day, tired feet at the end of the day. Other causes of arch and heel pain include arthritis, infection, fractures and sprains, and even certain systemic diseases. Since there are multiple possible causes, you should see your podiatrist for a thorough evaluation if you are experiencing arch or heel pain that does not respond quickly to early treatment.
Diagnosis
A patient is asked to step with full body weight on the symptomatic foot, keeping the unaffected foot off the ground. The patient is then instructed to "raise up on the tip toes" of the affected foot. If the posterior tibial tendon has been attenuated or ruptured, the patient will be unable to lift the heel off the floor and rise onto the toes. In less severe cases, the patient will be able to rise on the toes, but the heel will not be noted to invert as it normally does when we rise onto the toes. X-rays can be helpful but are not diagnostic of the adult acquired flatfoot. Both feet, the symptomatic and asymptomatic - will demonstrate a flatfoot deformity on x-ray. Careful observation may show a greater severity of deformity on the affected side.
Non Surgical Treatment
Rest is the most important thing you can do. Stay off your feet, or use a cane. Gently apply ice to the arch for at least 30 minutes, and repeat every 3 or 4 hours. Apply mild compression to the foot. Use a Fabriform PSC Foot and Ankle Strap to help support the arch, reduce swelling, and relieve pain and fatigue. This strap is easy to apply and adjust for a custom fit. Low profile allows it to fit in any shoe. Allows you to apply just the right amount of arch support/compression for your foot. Before stepping down after sleeping or resting, stretch the arch of your foot by pulling up on the ball of the foot and toes, as far as you comfortably can; hold the foot in this position for ten seconds. Repeat at least ten times. Consideration should also be given to the use of night splints. These are very effective for stretching the plantar fascia to relieve first weight bearing pain.

Surgical Treatment
If you have pain that has not been responsive to other treatments, there is a new non-surgical treatment that was recently approved by the FDA. ESWT (extracorporeal shockwave therapy) uses strong electrohydraulic acoustic (sound) energy that triggers the body?s natural repair mechanism. This treatment method is safe, effective and requires a very short recovery period compared to older surgical techniques.
Prevention
It is possible to prevent arch pain by wearing well-fitting shoes while performing any physical activity. Many times doctors will suggest a therapeutic shoe with a higher heel to relieve the pressure on the achilles tendon and also the arch muscle (plantar fasciitis). People with arch pain suffer from regular flare-ups of pain. However there is no risk to others as this is not a contagious condition.
Stretching Exercises
Flexibility is important in preventing injuries. With a simple stretching exercise, you can rehabilitate the muscles of your foot to relieve arch pain and prevent future injuries. This simple exercise by Tammy White and Phyllis Clapis for Relay Health is a good way to strengthen your foot muscles and stretch your plantar fascia. Sit in a chair and cross one foot over your other knee. Grab the base of your toes and pull them back toward your leg until you feel a comfortable stretch. Hold 15 seconds and repeat three times. When you can stand comfortably on your injured foot, you can begin standing to stretch the plantar fascia at the bottom of your foot.
Arch pain is felt on the underside of your foot between the heel and ball. The purpose of the arch is to transfer your body weight from heel to toe, and pain is the result when the arch doesn?t function properly. Your foot actually contains two arches: the longitudinal arch which runs the length of your foot, and the transverse arch (also known as the metatarsal arch) which spans the width of your foot. There are 24 bones which create the arches and these bones are held together through their unique interlocking shapes and ligaments. The muscles and the plantar fascia (a broad band of fibrous tissue which runs from the heel to the toes) provide secondary support, and fat pads help to absorb impact and bear your weight. If any of these structures or their interaction are damaged or faulty, arch pain may occur. The most common cause of arch pain is plantar fasciitis, an inflammation of the plantar fascia. You may also suffer arch pain if you have a structural imbalance in your foot or suffer from arthritis. But arch pain may also result from stepping on a rock or when someone steps on your foot. This force may cause an injury such as a bone fracture or damage to the supporting muscles, ligaments, or tendons underneath your foot.
Causes
Spending a lot of time on your feet. Especially when you are not used to doing so. For example you may have started a new job such as waiting tables where you are on your feet all day and wake up the next day with sore feet. This is a sign of damage and over time could lead to plantar fasciitis. Being Over-Weight. Never an easy topic to discuss but in simple terms, the heavier you are, the greater the burden on your feet. There are times when you're walking when your entire body weight is borne on one leg and therefore one foot, placing great strain on the plantar fascia. Wearing shoes with poor arch support or cushioning. A tight Achilles tendon. This is the big tendon at the bottom of your calf muscles above your heel. If this is excessively tight this can affect your ability to flex your ankle and make you more likely to damage your plantar fascia. Suddenly changing your exercise routine. Using running as an example if you suddenly run many more miles than your are used to or change to a new running surface e.g. grass to tarmac - these factors can put excessive strain on the plantar fascia and lead to plantar fasciitis. All of these risk factors ultimately lead to a specific change in foot structure. The term given is over-pronation and this basically describes rolling in of the foot and lowering of the arches. It is this change that excessively elongates the plantar fascia which can lead to plantar fasciitis.
Symptoms
Common symptoms of plantar fasciitis include pain in the morning when you first get out of bed, pain and stiffness when you start to walk after sitting for a while, increasing arch or heel pain toward the end of the day, tired feet at the end of the day. Other causes of arch and heel pain include arthritis, infection, fractures and sprains, and even certain systemic diseases. Since there are multiple possible causes, you should see your podiatrist for a thorough evaluation if you are experiencing arch or heel pain that does not respond quickly to early treatment.
Diagnosis
A patient is asked to step with full body weight on the symptomatic foot, keeping the unaffected foot off the ground. The patient is then instructed to "raise up on the tip toes" of the affected foot. If the posterior tibial tendon has been attenuated or ruptured, the patient will be unable to lift the heel off the floor and rise onto the toes. In less severe cases, the patient will be able to rise on the toes, but the heel will not be noted to invert as it normally does when we rise onto the toes. X-rays can be helpful but are not diagnostic of the adult acquired flatfoot. Both feet, the symptomatic and asymptomatic - will demonstrate a flatfoot deformity on x-ray. Careful observation may show a greater severity of deformity on the affected side.
Non Surgical Treatment
Rest is the most important thing you can do. Stay off your feet, or use a cane. Gently apply ice to the arch for at least 30 minutes, and repeat every 3 or 4 hours. Apply mild compression to the foot. Use a Fabriform PSC Foot and Ankle Strap to help support the arch, reduce swelling, and relieve pain and fatigue. This strap is easy to apply and adjust for a custom fit. Low profile allows it to fit in any shoe. Allows you to apply just the right amount of arch support/compression for your foot. Before stepping down after sleeping or resting, stretch the arch of your foot by pulling up on the ball of the foot and toes, as far as you comfortably can; hold the foot in this position for ten seconds. Repeat at least ten times. Consideration should also be given to the use of night splints. These are very effective for stretching the plantar fascia to relieve first weight bearing pain.
Surgical Treatment
If you have pain that has not been responsive to other treatments, there is a new non-surgical treatment that was recently approved by the FDA. ESWT (extracorporeal shockwave therapy) uses strong electrohydraulic acoustic (sound) energy that triggers the body?s natural repair mechanism. This treatment method is safe, effective and requires a very short recovery period compared to older surgical techniques.
Prevention
It is possible to prevent arch pain by wearing well-fitting shoes while performing any physical activity. Many times doctors will suggest a therapeutic shoe with a higher heel to relieve the pressure on the achilles tendon and also the arch muscle (plantar fasciitis). People with arch pain suffer from regular flare-ups of pain. However there is no risk to others as this is not a contagious condition.
Stretching Exercises
Flexibility is important in preventing injuries. With a simple stretching exercise, you can rehabilitate the muscles of your foot to relieve arch pain and prevent future injuries. This simple exercise by Tammy White and Phyllis Clapis for Relay Health is a good way to strengthen your foot muscles and stretch your plantar fascia. Sit in a chair and cross one foot over your other knee. Grab the base of your toes and pull them back toward your leg until you feel a comfortable stretch. Hold 15 seconds and repeat three times. When you can stand comfortably on your injured foot, you can begin standing to stretch the plantar fascia at the bottom of your foot.
Flexible Flat Foot In Adults
Overview
Posterior tibial tendon insufficiency (also called posterior tibial tendon dysfunction or adult acquired flatfoot) has been named literally after failure of the posterior tibial tendon. However, the condition is caused not only by the progressive failure of the posterior tibial tendon; it is also failure of associated ligaments and joints on the inner side of the ankle and foot. This results in collapse of the arch of the foot, along with the deformity which most often becomes the debilitating problem in its later stages. While at the beginning the common symptom is pain over the tendon in the inner part of the hindfoot and midfoot, later on it is the deformity that can threaten a person?s ability to walk. Just as the tendon degenerates and loses its function, other soft tissue on the same inner side of the foot - namely the ligaments - degenerate and fail. Ligaments are responsible for holding bones in place, and when they fail, bones shift to places where they shouldn?t; deformity is the result. The deformity causes malalignment, leading to more stress and failure of the ligaments. 
Causes
As discussed above, many health conditions can create a painful flatfoot. Damage to the posterior tibial tendon is the most common cause of AAFD. The posterior tibial tendon is one of the most important tendons of the leg. It starts at a muscle in the calf, travels down the inside of the lower leg and attaches to the bones on the inside of the foot. The main function of this tendon is to hold up the arch and support your foot when you walk. If the tendon becomes inflamed or torn, the arch will slowly collapse. Women and people over 40 are more likely to develop problems with the posterior tibial tendon. Other risk factors include obesity, diabetes, and hypertension. Having flat feet since childhood increases the risk of developing a tear in the posterior tibial tendon. In addition, people who are involved in high impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use. Inflammatory arthritis, such as rheumatoid arthritis, can cause a painful flatfoot. This type of arthritis attacks not only the cartilage in the joints, but also the ligaments that support the foot. Inflammatory arthritis not only causes pain, but also causes the foot to change shape and become flat. The arthritis can affect the back of the foot or the middle of foot, both of which can result in a fallen arch.
Symptoms
Not everyone with adult flatfoot has problems with pain. Those who do usually experience it around the ankle or in the heel. The pain is usually worse with activity, like walking or standing for extended periods. Sometimes, if the condition develops from arthritis in the foot, bony spurs along the top and side of the foot develop and make wearing shoes more painful. Diabetic patients need to watch for swelling or large lumps in the feet, as they may not notice any pain. They are also at higher risk for developing significant deformities from their flatfoot.
Diagnosis
The diagnosis of posterior tibial tendon dysfunction and AAFD is usually made from a combination of symptoms, physical exam and x-ray imaging. The location of pain, shape of the foot, flexibility of the hindfoot joints and gait all may help your physician make the diagnosis and also assess how advanced the problem is.
Non surgical Treatment
What are the treatment options? In early stages an orthotic that caters for a medially deviated subtalar joint ac-cess. Examples of these are the RX skive, Medafeet MOSI device. Customised de-vices with a Kirby skive or MOSI adaptation will provide greater control than a prefabricated device. If the condition develops further a UCBL orthotic or an AFO (ankle foot orthotic) could be necessary for greater control. Various different forms of surgery are available depending upon the root cause of the issue and severity. 
Surgical Treatment
For patients with a more severe deformity, or significant symptoms that do not respond to conservative treatment, surgery may be necessary. There are several procedures available depending on the nature of your condition. Ligament and muscle lengthening, removal of inflamed tendon lining, transferring of a nearby tendon to re-establish an arch, and bone realignment and fusion are examples of surgical options to help with a painful flatfoot condition. Surgery can be avoided when symptoms are addressed early. If you are feeling ankle pain or notice any warmth, redness or swelling in your foot, contact us immediately. We can create a tailored treatment plan to resolve your symptoms and prevent future problems.
Achilles Tendon Repair Cast Iron
Overview  The Achilles tendon is the soft tissue located in the heel which connects calf muscle to the heel bone allowing the body to perform certain activities such as rising on the tip toes and pushing off when running or walking. Achilles tendon tears occur when the tendon becomes torn through excessive pressure put on the area which the tendon is unable to withstand. Tears are most commonly found when suddenly accelerating from a standing position and therefore is often seen in runners and athletes involved in racquet sports. A tear can also occur when a continuous force is being put on the heel through prolonged levels of activity and overuse however this can also occur as a result of sudden impact or force to the area common in contact sports such as rugby and hockey. Although Achilles tendon tears can range in their severity, a rupture is the most serious form of tear and involves a completely torn tendon. This injury is more common in patients in their 30?s and 40?s. Causes The tendon usually ruptures without any warning. It is most common in men between the ages of 40-50, who play sports intermittently, such as badminton and squash. There was probably some degeneration in the tendon before the rupture which may or may not have been causing symptoms. Symptoms Tendon strain or tendon inflammation (tendonitis) can occur from tendon injury or overuse and can lead to a rupture. Call your doctor if you have signs of minor tendon problems. Minor tenderness and possible swelling increases with activity. There is usually no specific event causing sudden pain and no obvious gap in the tendon. You can still walk or stand on your toes. Acute calf pain and swelling can indicate a tear or partial tear of the Achilles tendon where it meets the calf muscle. You may still be able to use that foot to walk, but you will need to see a specialist such as an orthopedic surgeon. Surgery is not usually done for partial tears. Sometimes special heel pads or orthotics in your shoes may help. Follow up with your doctor to check for tendonitis or strain before resuming activity, because both can increase the risk of tendon rupture. Any acute injury causing pain, swelling, and difficulty with weight-bearing activities such as standing and walking may indicate you have a tear in your Achilles tendon. Seek prompt medical attention from your doctor or emergency department. Do not delay! Early treatment results in better outcome. If you have any question or uncertainty, get it checked. Diagnosis A detailed history, and examination by an appropriately qualified health professional, will allow a diagnosis to be made. An ultrasound or MRI scan can confirm the diagnosis. Other causes of symptoms in the area, such as those referred from the lumbar spine and local infection, should be excluded. Non Surgical Treatment Your doctor may advise you to rest your leg and keep the tendon immobile in a plaster cast while it heals. Or you may need to have an operation to treat an Achilles tendon rupture. The treatment you have will depend on your individual circumstances, such as your age, general health and how active you are. It will also depend on whether you have partially or completely torn your tendon. If you have a partial tear, it might get better without any treatment. Ask your doctor for advice on the best treatment for you. If you need pain relief, you can take over-the-counter painkillers such as paracetamol or ibuprofen. Always read the patient information that comes with your medicine and if you have any questions, ask your pharmacist for advice.
The Achilles tendon is the soft tissue located in the heel which connects calf muscle to the heel bone allowing the body to perform certain activities such as rising on the tip toes and pushing off when running or walking. Achilles tendon tears occur when the tendon becomes torn through excessive pressure put on the area which the tendon is unable to withstand. Tears are most commonly found when suddenly accelerating from a standing position and therefore is often seen in runners and athletes involved in racquet sports. A tear can also occur when a continuous force is being put on the heel through prolonged levels of activity and overuse however this can also occur as a result of sudden impact or force to the area common in contact sports such as rugby and hockey. Although Achilles tendon tears can range in their severity, a rupture is the most serious form of tear and involves a completely torn tendon. This injury is more common in patients in their 30?s and 40?s. Causes The tendon usually ruptures without any warning. It is most common in men between the ages of 40-50, who play sports intermittently, such as badminton and squash. There was probably some degeneration in the tendon before the rupture which may or may not have been causing symptoms. Symptoms Tendon strain or tendon inflammation (tendonitis) can occur from tendon injury or overuse and can lead to a rupture. Call your doctor if you have signs of minor tendon problems. Minor tenderness and possible swelling increases with activity. There is usually no specific event causing sudden pain and no obvious gap in the tendon. You can still walk or stand on your toes. Acute calf pain and swelling can indicate a tear or partial tear of the Achilles tendon where it meets the calf muscle. You may still be able to use that foot to walk, but you will need to see a specialist such as an orthopedic surgeon. Surgery is not usually done for partial tears. Sometimes special heel pads or orthotics in your shoes may help. Follow up with your doctor to check for tendonitis or strain before resuming activity, because both can increase the risk of tendon rupture. Any acute injury causing pain, swelling, and difficulty with weight-bearing activities such as standing and walking may indicate you have a tear in your Achilles tendon. Seek prompt medical attention from your doctor or emergency department. Do not delay! Early treatment results in better outcome. If you have any question or uncertainty, get it checked. Diagnosis A detailed history, and examination by an appropriately qualified health professional, will allow a diagnosis to be made. An ultrasound or MRI scan can confirm the diagnosis. Other causes of symptoms in the area, such as those referred from the lumbar spine and local infection, should be excluded. Non Surgical Treatment Your doctor may advise you to rest your leg and keep the tendon immobile in a plaster cast while it heals. Or you may need to have an operation to treat an Achilles tendon rupture. The treatment you have will depend on your individual circumstances, such as your age, general health and how active you are. It will also depend on whether you have partially or completely torn your tendon. If you have a partial tear, it might get better without any treatment. Ask your doctor for advice on the best treatment for you. If you need pain relief, you can take over-the-counter painkillers such as paracetamol or ibuprofen. Always read the patient information that comes with your medicine and if you have any questions, ask your pharmacist for advice.  Surgical Treatment Unlike other diseases of the Achilles tendon such as tendonitis or bursitis, Achilles tendon rupture is usually treated with surgical repair. The surgery consists of making a small incision in the back part of the leg, and using sutures to re-attach the two ends of the ruptured tendon. Depending on the condition of the ends of the ruptured tendon and the amount of separation, the surgeon may use other tendons to reinforce the repair. After the surgery, the leg will be immobilized for 6-8 weeks in a walking boot, cast, brace, or splint. Following this time period, patients work with a physical therapist to gradually regain their range of motion and strength. Return to full activity can take quite a long time, usually between 6 months and 1 year.
Surgical Treatment Unlike other diseases of the Achilles tendon such as tendonitis or bursitis, Achilles tendon rupture is usually treated with surgical repair. The surgery consists of making a small incision in the back part of the leg, and using sutures to re-attach the two ends of the ruptured tendon. Depending on the condition of the ends of the ruptured tendon and the amount of separation, the surgeon may use other tendons to reinforce the repair. After the surgery, the leg will be immobilized for 6-8 weeks in a walking boot, cast, brace, or splint. Following this time period, patients work with a physical therapist to gradually regain their range of motion and strength. Return to full activity can take quite a long time, usually between 6 months and 1 year.